
Skin Darkening Hormone: MSH, Melasma, and What Causes Hyperpigmentation

Dr. Matthew Olesiak, MD, is the Chief Medical Director at SANESolution, a renowned wellness technology company dedicated to providing evidence-based solutions for optimal living. Dr. Olesiak earned his medical degree from the prestigious Jagiellonian University Medical College in Kraków, Poland, where he developed a strong foundation in medicine.
The primary skin darkening hormone is melanocyte-stimulating hormone (MSH), a peptide produced in the pituitary gland that directly signals melanocytes to produce more melanin. When MSH levels rise, whether from pregnancy, adrenal disorders, or hormonal shifts during menopause, skin pigmentation increases, sometimes dramatically. But MSH doesn’t act alone. Other hormones like adrenocorticotropic hormone (ACTH), estrogen, and progesterone all play crucial roles in how much melanin your body produces and where dark patches appear. Understanding these hormones is the first step toward managing hyperpigmentation effectively.
I’ve seen patients walk into my office convinced their dark spots were just sun damage, only to discover an underlying hormonal imbalance was the real driver. The skin is an endocrine organ, and it responds to hormonal signals just like your thyroid, adrenal glands, and reproductive system do. And that means skin darkening can sometimes be the very first visible sign of a systemic condition that warrants further investigation.
What Is Melanocyte-Stimulating Hormone (MSH)?
Melanocyte-stimulating hormone belongs to a family of peptide hormones derived from a precursor molecule called pro-opiomelanocortin (POMC). The pituitary gland, a pea-sized structure at the base of the brain, cleaves POMC into several active hormones, including alpha-MSH (α-MSH), beta-MSH, gamma-MSH, and ACTH. Alpha-MSH is the most potent form for skin pigmentation.
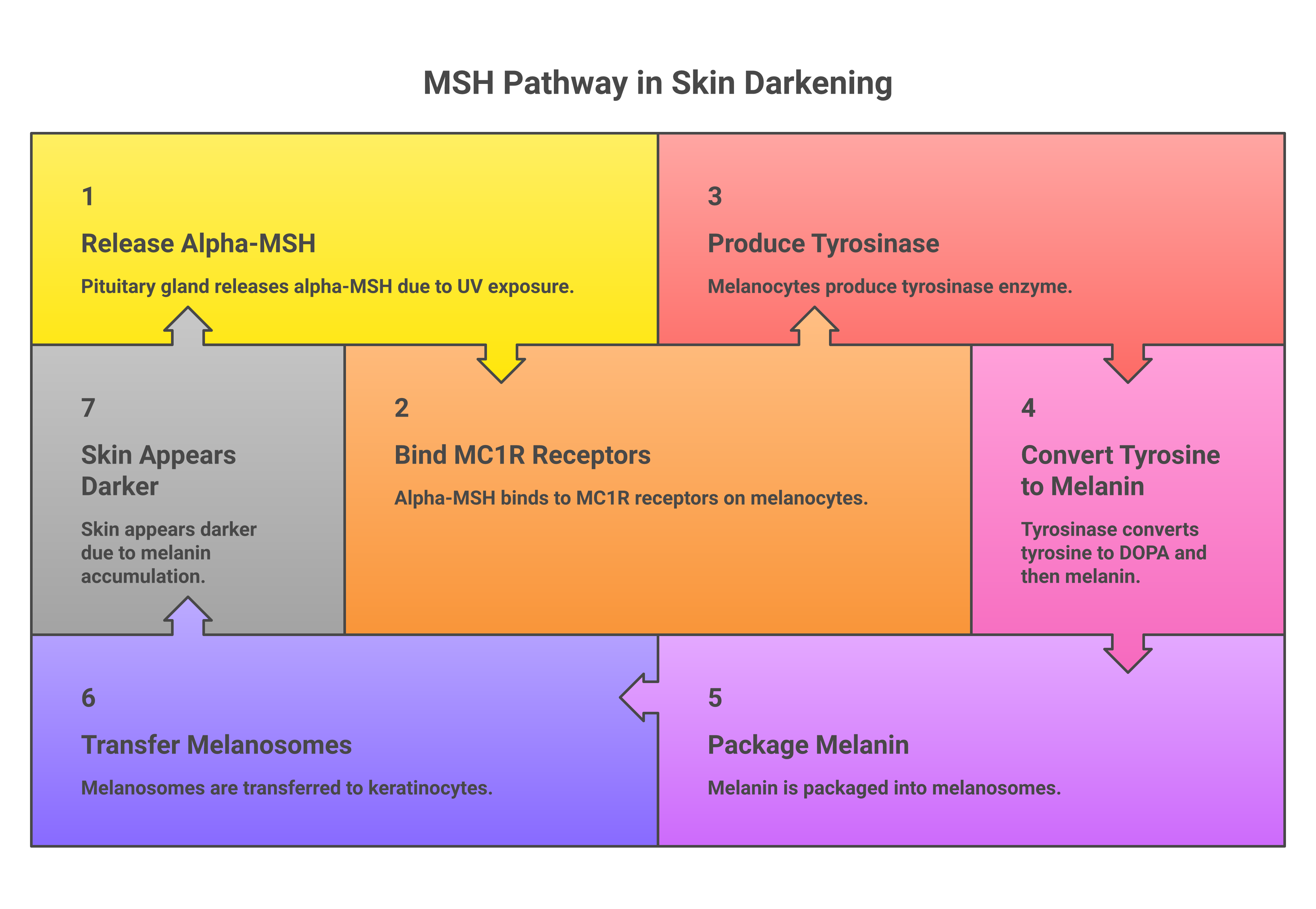
Here’s what happens at the cellular level: MSH circulates through the bloodstream and binds to melanocortin 1 receptors (MC1R) on the surface of melanocytes. These specialized skin cells sit in the basal layer of the epidermis. Once MSH docks onto MC1R, it triggers an enzyme called tyrosinase, which catalyzes the production of melanin from the amino acid tyrosine. The melanin is then packaged into structures called melanosomes and transferred to neighboring keratinocytes, making the skin visibly darker as melanin accumulates, the cells that make up most of the skin’s surface.
This entire process serves a protective function. Melanin absorbs harmful UV rays and shields DNA from ultraviolet radiation damage, reducing the risk of skin cancer. Without this protection, UV exposure can lead to cellular mutations. That’s why sun exposure naturally triggers more melanin production. Your body ramps up its defenses against sunlight. But when hormones push melanin production beyond what UV exposure alone would cause, the result is a pigmentation problem: hyperpigmentation: dark patches, uneven skin tone, and areas of skin color that don’t fade with standard sun protection.
MSH also plays roles beyond pigmentation. A study published in the Journal of Clinical Investigation found that MSH suppresses appetite through receptors in the hypothalamus, reduces inflammation throughout the body, and has a measurable impact on mood and sexual behavior. Multiple studies confirm these broader functions, which explain why hormonal disorders affecting MSH rarely produce skin changes alone. They typically come with a constellation of other symptoms.
How ACTH Drives Skin Darkening
Because ACTH and MSH share the same precursor molecule (POMC), any condition that elevates ACTH levels will simultaneously increase MSH, increasing melanin production along with it. This is one of the most clinically important connections in dermatology and endocrinology.
ACTH’s primary job is telling the adrenal glands to produce cortisol, the body’s main stress hormone. When cortisol levels drop (as happens in adrenal insufficiency), the pituitary gland compensates by pumping out more ACTH. And because POMC gets cleaved into both ACTH and MSH simultaneously, excess ACTH always means excess MSH. The result? Diffuse skin darkening, especially in areas exposed to friction, sun, or pressure.
This mechanism explains why Addison’s disease (primary adrenal insufficiency) causes such characteristic skin changes. Patients often develop a distinctive bronze or tan appearance in:
- Skin creases of the palms and soles
- Recent scars and surgical sites
- Gums and mucous membranes inside the mouth
- Knuckles, elbows, and knees
- Areas exposed to sunlight (face, neck, forearms)
About 90% of patients with Addison’s disease develop hyperpigmentation before diagnosis, according to published case reviews in the medical literature. The skin darkening is often the symptom that finally prompts a person to seek medical advice, sometimes after years of unexplained fatigue, weight loss, and low blood pressure.
High cortisol itself doesn’t directly darken skin. But in Cushing’s syndrome caused by a pituitary tumor (Cushing’s disease specifically), the tumor secretes excessive ACTH, which again drives MSH production upward. Patients with ACTH-dependent Cushing’s may develop darkened skin alongside the more recognizable features of cortisol excess: moon face, central weight gain, and muscle weakness.
Estrogen, Progesterone, and Skin Pigmentation
Estrogen and progesterone are the underlying hormones responsible for melasma (the brown or gray-brown patches that appear on the cheeks, forehead, nose, and upper lip). Melasma affects an estimated 15-50% of pregnant women, making it one of the most common skin changes during pregnancy. Many women notice these dark patches for the first time during their second trimester and about 10-25% of women taking birth control pills or hormone replacement therapy.
The mechanism works differently from MSH-driven pigmentation. Estrogen and progesterone do more than stimulate melanocytes. They actually increase the number of melanocortin receptors on those cells, making those cells hyperresponsive to any melanin-stimulating signal. Even normal levels of MSH produce outsized effects when estrogen levels are elevated. This is why melasma typically develops during periods of hormonal change:
- Pregnancy (chloasma, or the “mask of pregnancy”), rising estrogen and progesterone levels during the second and third trimesters increase melanin production, often creating symmetrical dark patches on the face. The linea nigra, a dark line running down the abdomen, develops through the same mechanism
- Oral contraceptives – combination birth control pills containing both estrogen and progesterone can trigger melasma in susceptible women, particularly those with darker skin tones or a family history of the condition
- Hormone replacement therapy – postmenopausal women on estrogen therapy sometimes develop new melasma patches or see old ones return
- Menopause transition – fluctuating estrogen levels during perimenopause create unpredictable pigmentation changes
What makes estrogen-driven hyperpigmentation particularly stubborn is the role of sun exposure. UV radiation and blue light from screens both worsen melasma by stimulating additional melanin production on top of what hormones are already causing. This combination of hormonal sensitivity and UV light is why melasma patches tend to darken in summer and lighten slightly in winter. But rarely disappear completely without intervention.
Research has found significantly higher estrogen receptor expression in melasma-affected skin compared to unaffected areas, including a study in the Journal of Drugs in Dermatology (2008) that demonstrated a qualitative increase in estrogen receptor expression in affected skin. These findings confirmed what dermatologists had long suspected: circulating hormone levels are only part of the equation. The way individual skin cells respond to those hormones at a local level determines whether melasma develops.
Medical Conditions That Cause Hormonal Skin Darkening
Several disorders can trigger widespread or localized skin darkening through hormonal pathways. Here’s how they compare:
| Condition | Hormone Involved | Pigmentation Pattern | Key Associated Symptoms |
|---|---|---|---|
| Addison’s Disease | Excess ACTH/MSH | Diffuse bronzing, gum darkening, creases | Fatigue, weight loss, low blood pressure, salt cravings |
| Cushing’s Disease (pituitary) | Excess ACTH/MSH | Generalized darkening | Moon face, central obesity, muscle weakness, mood disorders |
| Melasma (pregnancy-related) | Estrogen + Progesterone | Symmetrical patches on face | Typically no other symptoms; resolves postpartum in some cases |
| Nelson’s Syndrome | Very high ACTH/MSH | Severe generalized darkening | History of bilateral adrenalectomy, pituitary tumor growth |
| Hyperthyroidism | Thyroid hormones (indirect) | Generalized or patchy darkening | Weight loss, rapid heart rate, heat intolerance, anxiety |
| PCOS | Insulin + androgens | Acanthosis nigricans (dark velvety patches) | Irregular periods, acne, excess hair growth (hirsutism), oily skin, hair thinning on the scalp |
Addison’s disease remains the classic example of hormonal hyperpigmentation. When the adrenal glands fail, cortisol drops, ACTH surges, and skin darkening follows. The affected areas typically include sun-exposed surfaces, friction points, and mucous membranes. About 1 in 100,000 people develop Addison’s disease, but diagnosis is often delayed by months or years because early symptoms, fatigue, muscle weakness, mood changes, are nonspecific.
Nelson’s syndrome is rare but striking. It occurs in patients who’ve had both adrenal glands removed (bilateral adrenalectomy) as treatment for Cushing’s syndrome. Without the adrenals to produce cortisol, the pituitary tumor that was driving Cushing’s disease grows unchecked, producing massive amounts of ACTH and MSH. The resulting skin darkening can be severe.
Thyroid disorders also affect pigmentation, though the mechanism is less direct. Hyperthyroidism increases metabolic rate throughout the body, and some patients develop generalized hyperpigmentation, particularly on sun-exposed areas. Hypothyroidism, conversely, can cause dry skin and a slightly yellowish tone from impaired carotenoid metabolism.
Polycystic ovary syndrome (PCOS) causes a specific type of darkening called acanthosis nigricans, characterized by dark, velvety patches that typically appear in the folds of the neck, armpits, and groin. This isn’t driven by MSH but by excess insulin, which stimulates skin cell growth and melanin production simultaneously. About 5-10% of women of reproductive age have PCOS, and people with insulin resistance are especially susceptible, and acanthosis nigricans is often one of the earliest visible signs.
Other Causes of Hyperpigmentation (Non-Hormonal)
Not all dark spots stem from hormonal imbalance. Other common causes include:
- Post-inflammatory hyperpigmentation (PIH) – dark marks left behind after acne, eczema, burns, or other skin injuries. Inflammation triggers melanocytes to overproduce melanin as the affected area heals. PIH is more common and more persistent in darker skin tones
- Sun damage – chronic UV exposure causes age spots (also called liver spots or solar lentigines). These flat brown marks appear on the face, hands, shoulders, and forearms after years of cumulative sun damage. Tanning beds accelerate their formation
- Medication side effects – certain drugs increase skin photosensitivity or directly deposit pigment. Common culprits include minocycline (used for acne), amiodarone, antimalarials, and some chemotherapy agents
- Vitamin deficiency – B12 deficiency and folate deficiency can both cause diffuse hyperpigmentation, particularly in the hands, feet, and oral mucosa. Low iron doesn’t directly darken skin but can cause a sallow, uneven appearance
- Genetics – your baseline melanin production is largely determined by genetic factors that contribute to your natural skin color. People with naturally darker skin, as well as darker hair and eyes, have more active melanocytes and produce eumelanin more efficiently, which provides better UV protection but also makes them more prone to hyperpigmentation disorders like melasma and PIH
How to Treat and Manage Hormonal Dark Spots
Treating hormonal hyperpigmentation requires a dual approach: address the underlying cause and use topical treatments to lighten existing dark patches. Without correcting the hormonal trigger, even the best skincare routine will produce only temporary results.
Address the Hormonal Root Cause
If Addison’s disease is the driver, cortisol replacement medicine (hydrocortisone or prednisone) typically reduces ACTH levels and gradually improves skin darkening over weeks to months. For melasma triggered by birth control pills, switching to a non-hormonal contraceptive method may allow patches to fade. For pregnant women with melasma, the condition often improves postpartum as estrogen and progesterone levels normalize, though about 30% of women find their melasma persists.
Thyroid disorders require appropriate medication, specifically levothyroxine for hypothyroidism, antithyroid drugs or other interventions for hyperthyroidism. PCOS management with insulin sensitizers like metformin can improve acanthosis nigricans by reducing circulating insulin levels.
Topical Treatments That Work
For the pigmentation itself, several evidence-based topical treatments can help lighten dark patches:
- Hydroquinone (2-4%), inhibits tyrosinase enzyme activity, reducing melanin production. The gold standard for skin lightening, but should be used in cycles (typically 3 months on, 1 month off) to avoid ochronosis, a bluish-gray discoloration. Avoid using hydroquinone without guidance from a dermatologist
- Retinoids (tretinoin, adapalene, retinol), accelerate cell turnover and distribute melanin more evenly. Work well in combination with hydroquinone. May cause initial dryness and irritation
- Niacinamide (vitamin B3, 5-10%), blocks melanosome transfer from melanocytes to keratinocytes. Gentler than hydroquinone with anti-inflammatory properties and benefits for oily skin and pores
- Vitamin C (L-ascorbic acid, 10-20%), an antioxidant that inhibits tyrosinase and provides sun protection. Works as both a treatment and prevention agent. Look for stabilized formulations with vitamin E for best results
- Alpha arbutin – a naturally derived tyrosinase inhibitor that’s safer for long-term use than hydroquinone. Effective at concentrations of 1-2%
- Azelaic acid (15-20%), reduces melanin production and inflammation. Particularly useful for patients who also have acne or rosacea. Safe during pregnancy
In-Office Procedures
When topical treatments alone aren’t enough, procedural options include chemical peels (glycolic acid, salicylic acid, or TCA peels), laser treatments using a device called a Q-switched laser or fractional laser, and microdermabrasion. These work by removing the outer layers of skin where excess melanin has accumulated, promoting new cell growth with more even pigment distribution.
A word of caution: aggressive treatments can actually worsen hyperpigmentation in darker skin tones through post-inflammatory responses. The reduction of pigment should always be approached gradually, especially for patients prone to PIH.
Prevention Tips for Hormonal Skin Darkening
Prevention is significantly easier than treatment for hormonal pigmentation changes. Here are evidence-based strategies that protect skin health:
- Apply sunscreen daily – broad spectrum sunscreen with SPF 30 or higher is non-negotiable. UV rays are the number one factor that worsens hormonal hyperpigmentation. Reapply every 2 hours when outdoors, and use sun protection even on cloudy days since up to 80% of UV radiation penetrates clouds
- Wear protective clothing – wide-brimmed hats, sunglasses to protect your eyes and the delicate skin around them, and UPF-rated clothing provide physical barriers against sunlight that sunscreen alone cannot match
- Limit blue light exposure – emerging research shows visible light from screens and LED bulbs can worsen melasma. Mineral sunscreens containing iron oxide offer some protection against blue light wavelengths
- Maintain a healthy diet rich in antioxidants, vitamins C and E, along with other antioxidants, help protect melanocytes from oxidative stress that can trigger overproduction of melanin
- Manage stress – chronic stress elevates cortisol and ACTH levels, which can worsen pigmentation through the POMC pathway discussed earlier. Stress management benefits more than your brain and mood. It directly impacts your skin
- Know your risk factors – if you have a family history of melasma, darker skin type (Fitzpatrick III-VI), or are starting hormone replacement therapy or oral contraceptives, proactive sun protection and a targeted skincare routine can prevent pigmentation from developing in the first place
How MSH, Skin Tanning, and Melatonin Are Connected
Many women and people in general confuse the skin tanning process with simple UV damage, but the hormones play a more complex role. When ultraviolet light hits your skin cells, keratinocytes release alpha-MSH (α-MSH) locally, independent of pituitary signaling. This localized alpha MSH production is your body’s first-line defense against DNA damage from the sun.
The development of a tan follows a predictable hormonal sequence. UV exposure triggers α-MSH release, which activates melanocytes through MC1R binding, stimulating melanin production over the next 48 to 72 hours. The melanin produced then migrates upward through the epidermis, resulting in visible skin tanning. People with more responsive MC1R receptors tan easily, while those with certain MC1R variants (common in fair-skinned individuals) produce pheomelanin instead of eumelanin, leading to sunburn rather than tanning.
Melatonin, often called the “sleep hormone,” has a less understood but important relationship with skin color. Despite the similar name, melatonin and melanin serve different functions. Melatonin is produced by the pineal gland and regulates sleep-wake cycles, but studies published in the International Journal of Molecular Sciences (2018) have found that melatonin also acts as an antioxidant in skin cells, potentially offering protection against UV-induced melanin overproduction. Some researchers are investigating whether melatonin supplements could help regulate hormone increases that contribute to hyperpigmentation, though this research remains preliminary.
Vitiligo: When MSH Signaling Fails
While hormonal changes cause skin darkening, the opposite condition also exists. Vitiligo is an autoimmune skin condition where the immune system attacks and destroys melanocytes, creating white patches where no melanin is produced. About 0.5 to 2% of the global population has vitiligo, according to the American Academy of Dermatology.
Understanding vitiligo helps clarify how MSH works. In vitiligo, even normal MSH levels cannot trigger melanin production because the target melanocytes are absent or dysfunctional. This is important context for anyone researching skin darkening hormones: the problem can exist on either end of the spectrum. Too much MSH activity (or hormonal sensitivity) leads to hyperpigmentation and dark patches. Too little melanocyte function leads to depigmentation. Some medicine used to treat vitiligo, such as narrowband UVB phototherapy, works partly by stimulating remaining melanocytes to produce melanin in response to UV-triggered MSH release.
Beyond prescription medicine, daily skincare products can support treatment of this skin condition. Use moisturizers with ingredients like ceramides or hyaluronic acid to maintain your skin barrier while using active treatments. Many women find that a consistent routine of gentle cleansing, targeted treatment, and moisturizing helps avoid irritation that can worsen pigmentation. Additionally, mineral sunscreens with sun protection factor (SPF) 50 provide better protection against both UV and visible light types compared to chemical formulas alone. The understanding of how hormonal changes impact skin color continues to evolve, and newer products combine multiple active ingredients to address both the hormonal root cause and the visible effects on skin tone.
When to See a Doctor About Skin Darkening
Not every instance of skin darkening needs medical attention. Mild melasma patches on the cheeks or occasional dark spots on the forehead can often be managed with consistent sun protection and over-the-counter topical treatments.
But certain patterns of skin darkening warrant prompt evaluation. Consult a doctor if you notice:
- Rapid, widespread darkening that appears over weeks rather than months, which could signal Addison’s disease or another endocrine disorder
- Darkening of gums, tongue, or inside the cheeks: mucous membrane pigmentation is a hallmark of excess ACTH
- Dark patches in skin creases, scars, or knuckles: these friction-point changes suggest systemic rather than localized causes
- Accompanying symptoms: unexplained fatigue, weight loss, low blood pressure, dizziness, salt cravings, or muscle weakness alongside skin changes
- New darkening after starting medication: several prescription drugs can cause pigmentation as a side effect
- Skin changes that don’t respond to treatment after 3-6 months of consistent care
A dermatologist can evaluate cosmetic pigmentation concerns and determine whether the cause is hormonal, sun-related, or post-inflammatory. If hormonal involvement is suspected, a referral to an endocrinologist for blood tests measuring cortisol, ACTH, thyroid hormones, and estrogen levels can identify the specific imbalance driving the changes. Early diagnosis is important, conditions like Addison’s disease are serious but highly treatable once identified.
Frequently Asked Questions
What hormone makes your skin darker?
Melanocyte-stimulating hormone (MSH) is the primary hormone responsible for skin darkening. It binds to receptors on melanocytes and stimulates the production of melanin, the pigment that determines skin color. ACTH, estrogen, and progesterone can also increase melanin production through different but overlapping mechanisms.
Can a hormonal imbalance cause dark spots on the face?
Yes. Hormonal imbalance is one of the most common causes of facial dark spots, particularly in women. Elevated estrogen and progesterone trigger melasma (sometimes called the mask of pregnancy), which causes symmetrical brown patches on the cheeks, forehead, nose, and upper lip. This commonly occurs during pregnancy, while taking oral contraceptives, or during menopause. Thyroid disorders and adrenal conditions can also cause facial pigmentation.
Does low iron cause skin to darken?
Low iron (iron deficiency anemia) doesn’t directly cause skin darkening through melanin overproduction. However, it can cause a pale, sallow complexion that makes existing pigmentation appear more noticeable. Severe iron deficiency may also cause a yellowish tint. Other nutrient deficiencies, particularly vitamin B12 and folate, can cause actual hyperpigmentation, especially on the hands, feet, and inside the mouth.
Can high cortisol cause dark skin?
High cortisol alone doesn’t darken skin. But the condition causing high cortisol matters. In Cushing’s disease (caused by a pituitary tumor), the tumor produces excess ACTH, which gets converted alongside MSH from the same POMC precursor. The excess MSH then darkens the skin. In Cushing’s syndrome caused by adrenal tumors or exogenous steroids, ACTH is actually suppressed. So skin darkening doesn’t occur.
How do you fix hormonal hyperpigmentation?
Fixing hormonal hyperpigmentation requires treating the underlying hormonal trigger while simultaneously using targeted topical treatments. For melasma, this often means combining sunscreen, hydroquinone or alpha arbutin, retinoids, and vitamin C. For Addison’s disease, cortisol replacement reduces ACTH and MSH levels over time. Chemical peels and laser treatments can supplement topical therapy for stubborn patches.
What does hormonal skin pigmentation look like?
Hormonal pigmentation typically appears as symmetrical brown, gray-brown, or tan patches on the face, most commonly on the cheeks, forehead, nose, and upper lip (the melasma pattern). In conditions like Addison’s disease, the darkening is more diffuse and affects creases, scars, gums, and sun-exposed surfaces. PCOS-related acanthosis nigricans looks different: dark, velvety, thickened skin in body folds like the neck, armpits, and groin.
Is skin darkening during pregnancy permanent?
In many cases, no. Pregnancy-related melasma and the linea nigra often fade within several months after delivery as estrogen and progesterone levels return to baseline. However, about 30% of women find that some degree of pigmentation persists long-term. Sun protection during and after pregnancy significantly improves the chances of complete resolution.
This information is for educational purposes only and does not constitute medical advice. Consult a qualified healthcare provider for diagnosis and treatment of any medical condition. Individual results may vary.

